A 36 year old female with Dengue Ns1 Antigen positive and IgG positive , viral Hepatitis
Unit 4 admission :
A 36 year old female house wife came to the hospital with complaints of
Fever since 5 days
Abdominal pain since 5 days
Nausea since 5 days
patient was apparently asymptomatic 5 days back. Then she complained of fever which is high grade , continuous ; not associated with chills and rigors . Relieved with medication .
No complaints of cold and cough . patient complaints of generalised weakness .
Patient complaints of nausea, vomiting 2- 3 episodes per day associated with food particles , non bilious , non blood tinged.
Patient complaints of abdominal pain in the umbilical region , which is squeezing type and relieved after vomiting . No complaints of loose stools or constipation . No c/o pedal edema, Facial puffiness . No c/o burning micturition .
No c/o chest pain, palpitations , syncopaal attacks . C/o sob grade 2. orthopnea and pnd absent.
C/o frontal headache which got subsided on medication. No c/o bleeding manifestations . she was a known case of hypothyroid on thyronorm 50 microgram po / od
Past History: No H/O of Diabetes , Hypertension, CAD, Asthma, Tuberculosis
Personal History:
Diet :Mixed
Appetite: lost
Sleep: adequate
Bowel and bladder habits : Regular
Addiction:No addictions
On examination:
Vitals:
PR: 100 bpm
Bp: 100/70 mm of hg
Spo2: 96% at RA
Grbs: 144 mg%
No pallor, Icterus, Cyanosis, Clubbing, lymphadenopathy, edema
Systemic examination:
Cvs:
S1 S2 present
No murmurs, no thrills
Rs:
Normal vesicular breath sounds heard
Abdomen:
Shape: scaphoid
Tenderness present in umbilical region, No palpable masses
Cns: NAD
Provisional diagnosis:
Dengue ( Ns1, IgG positive with Thrombocytopenia (resolving) with viral hepatitis
Investigations:
On 12/ 08/ 21:
Hemogram:

















On 14/08/21:


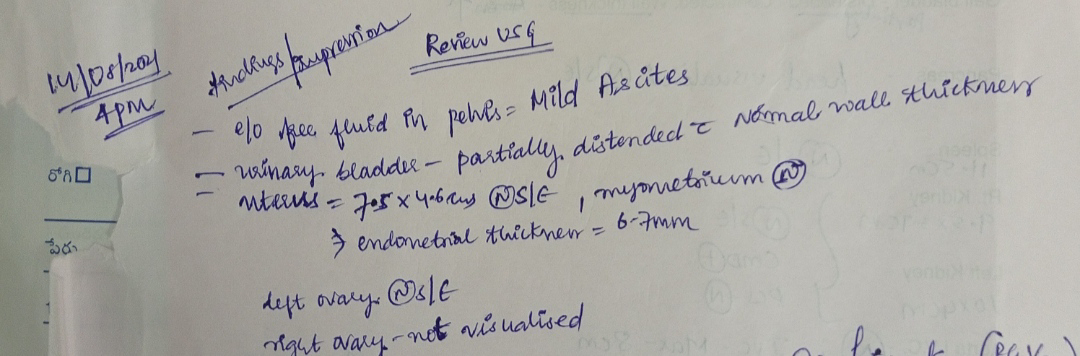
Obg referral for PV clots:


On 15/8/21:

On 16/8/21:

Ophthalmology referral for blackish discoloration of left eye:


On 17/8/21:


Fever chart:

Treatment given:
Day 1:
1. IVF - 2 NS, 2 RL @ 125ml/hr
2. Inj. PAN 40mg IV/OD
3. Inj. ZOFER 4mg IV/TID
4. Temperature charting 4th hourly
5. BP/PR/RR/SPO2 monitoring 2nd hourly
6. Strict I/O charting
7. Watch for bleeding manifestations
Day 2:
1. IVF - 2 NS, 2 RL @ 100ml/hr
2. Inj. PAN 40mg IV/OD
3. Inj. ZOFER 4mg IV/TID
4. Temperature charting 4th hourly
5. BP/PR/RR/SPO2 monitoring 2nd hourly
6. Strict I/O charting
7. Watch for bleeding manifestations
Day 3:
1. Plenty of oral fluids
2. Tab. PAN 40mg PO/OD
3. Tab. MVT PO/OD
4. Strict I/O charting
5. BP/PR/RR/SPO2 charting 4th hourly
6. IVF - 2NS, 1RL @75ml/hr
7. Syp. Cremaffin plus PO/HS 15ml
Day 4:
1. Plenty of oral fluids
2. Tab. PAN 40mg PO/OD
3. Tab. MVT PO/OD
4. Strict I/O charting
5. BP/PR/RR/SPO2 charting 4th hourly
6. IVF - 2NS, 1RL @75ml/hr
7. Syp. Cremaffin plus PO/HS 15ml
Day 5:
1. Plenty of oral fluids
2. Tab. PAN 40mg PO/OD
3. Tab. MVT PO/OD
4. Strict I/O charting
5. BP/PR/RR/SPO2 Charting 4th hourly
6. IVF - 2NS, 1RL @75ml/hr
7. Syp. Cremaffin plus PO/HS 15ml
8. Tab. THYRONORM 50mcg PO/OD
Day 6:
1. Plenty of oral fluids
2. Tab. PAN 40mg PO/OD
3. Tab. MVT PO/OD
4. Tab. PCM 650mg PO/SOS
5. Tab. THYRONORM 50mg PO/OD
6. Strict I/O charting
7. Tab. PAUSE MF 500mg PO/BD
8. Tab. MEDROXY PROGESTERONE 5mg PO/TID
Day 7:
1. Plenty of oral fluids
2. Tab. PAN 40mg PO/OD
3. Tab. MVT PO/OD
4. Tab. PCM 650mg PO/SOS
5. Tab. THYRONORM 50mg PO/OD
6. Strict I/O charting
7. Tab. PAUSE MF 500mg PO/BD
8. Tab. MEDROXY PROGESTERONE 5mg PO/TID
COURSE IN HOSPITAL:
A36 year old female came to hospital on 12/08/21 with complaints of fever, abdominal pain, nausea. IV fluids were started. Her platelet count on day of admission - 1.3 lakhs/cumm. Later on 14/08/21 platelet count was 60,000. On 15/08/21 platelet count was 45000. On 16/8/21 platelet count was 85000. On 17/8/21 platelet count was 1.6 lakhs/cumm. After two days of admission she complained of bleeding clots PV and obg referral was taken and medications were prescribed. Patient had H/O head trauma after admission in the hospital (5 days back) and blackish discoloration in the frontal region . No H/o loss of consciousness, seizures, patient had blackish discoloration of left eye , ophthalmology referral was taken and the fundus was normal. CT was done in view of head injury and it was normal. As her symptoms were relieved and platelet count is increased we planned her discharge today i.e. on 18/08/21.